|
12. ULUSAL KOLON VE REKTUM CERRAHISI KONGRESI 19.05.2009 – 24.05.2009 ANTALYA
Prof. Dr. Nihat BENGİSU
Bengisu Proktoloji Genel Cerrahi Uzmanı
Dr. Serap PAMAK
Haseki Hastanesi Genel Cerrahi Ana Bilim Dalı
Ar. Gör.
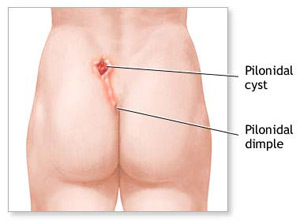
PİLONİDAL HASTALIĞIN TEKRARLAMA NEDENLERİ VE KORUYUCU YÖNTEMLER
GİRİŞ
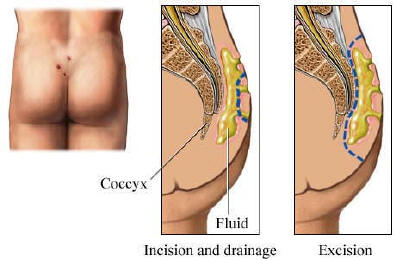
Pilonidal sinus cerrahisinde %20’lere varan nükslerin olması, etiopatogenezi ve cerrahi yöntemleri hep tartışılır kılmıştır. Fenol ile konservativ tedaviden radikal Limberg’e kadar yaklaşık 15 çeşit tedavi önerilmiştir. Bizler 1985’ten 2001’e kadar 1500 kadar hastada etioloji soruşturması yanında tedavide sklerotik etkisi nedeni ile sadece %80 Fenol uygulayarak %86 başarı; 2001’den 2005’e kadar litik etkisi nedeni ile %20 Gümüş nitrat ve küretaj uygulayarak %92 başarıya ulaşmış idik. Bu kez 2005’ten beri etiyopatogenezi ve nüksleri daha iyi sogulamayı, sklerozan ajan kullanmadan doğrudan granulasyon küretajını ve mikro pit eksizyonu ile daha iyi sonuç almayı amaçladık.
MATERİAL VE METOD
Mart 2005-Mart 2009 yılları arasında 2914 hastada koruyucu yöntemler olarak:A) Evre 1-2-3 olanlara lokal anestezi altında sinus veya fistül içi küretajı + pit eksizyonu
B) Birlikte gerekiyorsa retrakte fossa eksizyonu
C) Vakaların %15 inde da kist membran ieksizyonu. Evre 4 olanlara küretaj + pit eksizyonu + sınırlı Lay-open.
E) Anatomi bozulmuşsa sınırlı düzeltici plastik yöntemler.
F) Mikroeksizyonlarda sütür yerine baskılı tampon uyguladık.
G) Kaykılık oturmayı kesin terk etmeyi.
H) Günde 3 kez bölgeyi elle veya pudra ile silmeyi.
İ)Derin oluğu string çamaşır ile korumayı önerdik.
BULGULAR
A-Kişisel ve edinsel etiyolojik nedenler
1- Kaykılık oturmaya bağlı pit veya follicle oluşumu: Hastaların %100’ünde bilgisayar önünde, büro veya sürücü koltuklarında uzun süreli kaykılık oturma alışkanlığı; %21 ‘inde belirgin koksiks ve bu durumlarda gerilen cilt ile birlikte genişleyen apokrin orifislerden serbest tüy ve kılların cilt altına itildiğini saptadık.
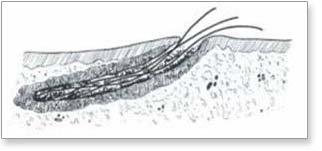
2- Kılların yivli ve kontamine yapısı: Kılların yüzeyi yılan derisi gibi pullu, yivli ve olduğu; bu sayede, orifis veya pit önüne denk düşmüş kılın içeriye ittirilince pisi pisi otu veya vida dinamiği ile mikroorifis ve klivajlardan yürütülebilir olduğunu; apokrin orifiste mikroenfeksiyon ve pit denilen 0,1-2 mm mikrokrater oluşturduğunu ve bu pitlerden yeni kıl girişlerinin kolaylaştığını,
3- Apokrin veya hidradenitis olasılığını
4- Derin intergluteal oluklarda hijyen kusurunu ve bunu string çamaşırın önlediğini saptadık.
B- Cerrahi nedenler
1-Yaranın açık bırakılması: Bu durumda zor ve geç iyileşen ince, fibrotik, fragil bir zeminde kolay fissür,
intertrigo ve ülserasyon gelişmektesp.
2- Limberg tipi bazı ameliyatlarda gergin bir prekoksigeal kemer ve kıl girişine uygun pitler oluşmakta.
3-Söz konusu kemerin distalinde derin fossa oluşumakta ve kıl, hav, ter ile dolup intertrigo, pyodermi ve ülsearsyona zemin hazırlanmakta
4-Postoperatif distal intergluteal yüzlerin yanaşık bırakılması halinde sürtünme ile dibe yürütülmesi kolaylaşmakta
SONUÇ VE YORUM
“Kıl girişi ter veya apokrin orifislerden oluşmakta ve büyük olasılıkla enfeksiyon ta baştan itibaren bir apokrin veya hidradenitistir” diye düşünüyoruz. Nitekim hastalık süresi 10 yılı
aşmış vakalarımızın % 62’sinde hidradenitis bulguları saptandı. Dolayısıyla süreç kronikleşmeden küretaj ve sadece pit eksizyonu; retrakte fossalara sınırlı plastik cerrahyi; koruyucu olarak koksiks üzerine oturmaktan kaçınmayı; günde üç kez oluğu silmeyi ;derin olukta intertrigo ve kıl yürüyüşünü önleyici string çamaşırı öneriyoruz.
|

|
|
Resim 1 (Foto 205-2):Bir sene önce pilonidal sinus tanısı ile flap rotasyon uygulanmış; ancak bir ay sonra akıntı yinelemiş olan hastanın muayenesinde rhomboid flap alt ucunda akıntılı bir pit (kıl girişi orifisi) ve bu yüzden zamanla oluşmuş retraktif fossa ve 7 cm proksimale uzanan kıl ve granulasyon dolu
trakt ve üst ucunda 3x7 mm bol akıntılı çıkış orifisi vardı.
|
|

|
|
Resim 2 (Foto 205-5):
Povidon iyod ile irrigasyondan sonra lokal anestezi altında (LAA) buşon küretleri ile trakt temizlendi. Pit ve iligili fossa eksize edilerek 5 adet sütürle kapatıldı. Proksimal çıkış orifisi drenaj için açık bırakıldı. Trakt eksizyonu yapılmadı, sadece baskılı tampon kondu ve bir hafta sonra sütürler alındı. Bu yöntemle retrakte fossalı 156 vaka, %97 başarı sağlandı.
|
|

|
|
Resim 3 (Foto 522-3):
Altı ay önce kuyruk sokumnda akıntı ile fark eden hastanın presakral olukta 3 adet ardışık, penetran pit ve 25 mm proksimal orta hatta 2x2 mm az granulasyonlu çıkış orifisi vardı. LAA, kıllar ve granulasyon kürete edildi. Proksimal orifisteki cilt epitelyumu ikişer mm’lik mikro eksizyon; distal ve ortadakiler ise dişçi kanal eğesi ile giderildi ve baskılı tampon kondu.
|
|

|
|
Resim 4 (Foto 522-4):
İki gün sonraki kontrolde orifisler veya mikro cerrahi yaralar iyileşmiş idi. Beş mm’den küçük mikro eksizyonlar ve pitler bu yöntemle sütürsüz iyileştiler. |
|

|
|
Resim 5 (Foto 526-3): Altı aydır kuyruk sokumunda az akıntı ve 1 haftadır da şişlik olan hastanın prekoksigeal gergin cilt üzerinde 3 adet ardışık penetran pit ve zeminde derinliği belirsiz enfekte sinus vardı. |
|

|
|
Resim 6 (Foto 526-6):
LAA 8 mm derinliğe uzanan, birbirinden bağımsız 3 adet sinusten 1cc pü ve pyojenik granulasyon ve 30 adet kıl ve 0,2 gr granulasyon kürete edildi. Pitlere mikroeksizyon ve baskılı tampon uygulandı. Oral antibiotik başlandı. İki ve 7 gün sonraki kontrollerde sorun bitmişti. |
25-29 MAYIS 2005 -AVRUPA CERRAHLARI CERRAHİ ARAŞTIRMA KONGRESİ
Nihat Bengisu
Serap Pamak
Erol Kisli
Sebahattin Aytekin
Proctology Office, Istanbul, TURKEY
CURATTAGE THE PILONIDAL SINUS-FISTULA,THEN EXCISE THE HAIR INPALNTING ENTRIES
INTRODUCTION
It has been already understood that the pilonidal sinus disease is an acquired, subcutaneous chronic infection secondary to hair inplantation it is not a congenital condition. So, the treatment must be more different, more simple, more conservative then the classical and complicated surgical methods with high morbidity.
THE ETIOPATHOLOGY OF THE PILONIDAL OF PILONIDAL SINUS MUST AS FOLLOWS
1-Before The Symptomatic Or Supurative Cyst Or Tract Formation,Some Epitelized 0,1x2 Mm Microtubules, Or Pits Are Formed On The Deep Midline Skin Of Intergluteal Cleft ,Of Some Juniors
2-The Pits May Be Formed Due To Repeated Streching, Pumping, Vacoom Or Some Micro Travma Against The Intergluteal Cleft At The Moment Of Sitting, Driving, Riding, Sporting Or Trawelling.
ETIOPATHOLOGY
 3- The pits are filled by cutaneous ceratin
plugs in the beginning then by the time, he hairs may inplant into the pits, by the similar mechanisms. 3- The pits are filled by cutaneous ceratin
plugs in the beginning then by the time, he hairs may inplant into the pits, by the similar mechanisms.
4- Each hair inplant sure will cary bacteria into pits,and may form microabscesses or cronical infection ,supurating fibrotic tracts or large pilonidal cysts, just under the skinand also every new hair may widen the pits and fasilitates more hair to enter
5-We have found the hairs to stay freely in the pilonidal tracts or sinus or loosely attached to the granulating tissue, sometimes embedded into the fibrotic sinus wall vertically, but we have found no hair follicles, nore thight binding to the floor and neitherhair passing out of the fibrotic capsula and also we have found no other skin accessories in and around of the tracts, nor in the previous large operations before 1985, nor in our current small operations.
6- The scaled surface of human hair, may
fascilitates itself to drill throug any pits or fistula or apocrine or sweat
gland openings, particularly on the midline of intergluteal sulcus and trawels
beneath of the skin, surprisingly to the cephalad way, like a tailed seed. (fig
1-2:asian and african hairs)
7- We have extracted files of cut hair belonging to the scalp in some cases, that is discarding the congenital theory.
8- All observations imply that the pilonidal sinus disease is an acquired, subcutaneous disease so we have abondoned the radical and large surgical treament due to high morbidities instead, we have introduced more conservative methods, having little morbidity.
MATERIAL AND METHOD
Between january 2003 and march 2005 we have treated 1132 patients with pilonidal sinus-fistula disease, aging from 15 to 55 years(male/female=20/1). We have treated the sclerotic and hidradenitic pilonidal fistulae, disseminated farther then 6 cm from the cleft by flaping and again we have resected the whole capsula of the nonsupurating cystic forms, larger than 2x2x2 cm through an 1-1,5 cm inscison and have sewed the residual cavities with 3/0 vicryl and the inscisions by 2-3 stiches of 5 / 0 monoflament stitches and exluded them to deal whitin a separate study.
AgNO3 INSTILLATION GROUP
 As we know, agno3 crystals or high consantrations more then %30 cauterize the granulating tissue in wounds with no pain. So we have introduced a model of concervative treatment based on cauterization and liquifying of the granulating tissue in the pilonidal sinus fistula, then curattage only. For agno3 treatment we have selected the fistulated pilonidal cases just around the cleft and unsupurated cystic forms smaller than 2x2x2 cm but no cases with large and deep retractive dimples which needed excision and sewing no shallow pits, no uncapsulated microcysts, nor supurated cystic forms to avoid pain and failure.
As we know, agno3 crystals or high consantrations more then %30 cauterize the granulating tissue in wounds with no pain. So we have introduced a model of concervative treatment based on cauterization and liquifying of the granulating tissue in the pilonidal sinus fistula, then curattage only. For agno3 treatment we have selected the fistulated pilonidal cases just around the cleft and unsupurated cystic forms smaller than 2x2x2 cm but no cases with large and deep retractive dimples which needed excision and sewing no shallow pits, no uncapsulated microcysts, nor supurated cystic forms to avoid pain and failure.
We have induced the treatment by a single instillation of %30-50 agno3 in distilated water, into pilonidal fistulaor sinus directly, without aenestesia. Afte then 3-24 hours, we have curattaged the cauterazied and liquified intrafistular or intra sinusal material under local aenestesia, as an office procedure we have excised the entries and sewed by a 5/0 monofilment stitch and left exits open to drainage. We have dressed the site tightly under pression to obviate any heamatoma or seroma formation.
CONSERVATIVE SURGICAL GROUP
We have treated 870 cases of nonsupurated and also supurated pilonidal sinüs or fistula, directly by curattaging the granulated tissues and hairs within the tractsthen excising and sewing the entries or pits under local aenestesia. To obviate the new hair inplantings we have excised all the entries and also the suspicious pits as in figure of rhomboids, as in size of 1x2 mm or 2x4 mm then sewed each, individualy , by a single u shape 5 / 0 suturewhile we have left open all the proximal or lateral exits for drainage in both groups.
We have inscised and curattaged the abscess forms thoroughly,and left open for drainage and again have excised and sewed the corresponding hair entries to obviate new inplantings. We have resected or unroofed the some old,sclerotic fistular forms and have excluded them to deal within a separate study. We have excised every retractive dimple ,or small fossa together with the etries within it, to obviate the accumulation of exfoliating hairs,which may induce the reccurrences. We have sutured every insicion by interrupted fine, 5/0 ,matress sutures, to obviate overlapings and skin suture cuts. We have dressed the operative area tightly under pressure to obviate seroma or heamotoma and sent to work or home, advising to restrict the harsch movements
and come back on the 3rd and 6th days to treat probable outcomes, like, wound infection or to take of sutures. To reduce the hair reinplantings, we have advised to sweep the cleft vigorously ,at least 3 times in a day,or shave the cleft until 30 years of age ,and advised never to sit at the semi- laying positions.
RESULTS
Almost all the cases were to be faty, hirshutic and long sitting juniors at the semi-laying positions. Many of them have did not left their sitting positions and habits yet, even of our hard warnings. Instillated %30-50 agno3 has liquified the granulating tissue and has widened and also made evident the pits and fistulaes, so has fascilitated to curattage and wash away off fistular matterial almost with no heamorage. Agno3 has no dissolving effect on hairs.
|
|
AgNO3 AND
CURATTAGE |
CURATTAGE AND
EXCISING PITS |
|
|
n 262 |
n 870 |
|
Wound infection |
23 (% 8.78) |
61 (%7.01) |
|
Wound dehisence |
- |
22 (%2.57) |
|
Heamatoma |
- |
24 (%2.75) |
|
Recurrence in 6 months |
12 (%1,37)? |
28 (%3.22) |
|
Recurrence in 30 months |
? |
? |
|
Duration of healing |
8 (5-20) days |
10 ( 5-27)
days. |
UNIVERSITY of KONYA SELÇUK
"40TH EUROPIAN SURGEON'S SURGICAL RESEARCH CONGRESS"
CURRATAGE OR UNROOFING OF THE PILONIDAL SINUS-TRACTS AFTER INSTILLATION OF AgNO3, THEN EXCISION OF THE INPLANTING PITZS WILL BE SUFFICIENT A TRILE OF 987 CASES
From January 2003 to January 2004 we have treated 987 cases with pilonidal sinüs disease grade 1-2-3. As we have shown with historical,surgical and histological studies ,that,the pilonidal sinüs disease is an acquired condition due to insertion of free hairs through the pitzs or follicles(hair entries) of the midline skinof the deep sacrococcygeal sulci, particularly of hairy, faty, long sitting, long travelling or riding young men, particularly in semilaying position against the bony, sacral basement. The pitzs may have been created by a repeated over streching of the midline skin and micropores, laterally by the buttocks and overcompressing of the thin skin in the cleft ,against of the bony structure of sacrococcygeal basement,at the time of long semilaying or semisitting pozisition. Finally the micropres widens enough for the passing or drilling of the free hairs throug of the pitzs right into the underlying tissues. If the treated patients by any surgical tehniquehave not been aware and if the predisposing conditions continue, postoperatively, surely the disease will repeat again in comming weeks or months. Since the surgical procedures like Limberg flaps,primary closing or marsupialization having high morbidity and recurrence rateswe have introduced a simple and effective techniqe depending on currataging of the Grade 1-2-3 pilonidal tracts and excising of the hair entries and retracting dimples around the entries if present.have little morbidity and reccurrence rates.
METHOD
Our procedure was based on instillation of 0,3-1 cc %30 AgN03 solution into Grade 1,2 and 3 hairy tracts,instead of Fenol or Metilen blue,in the first step, without local aenesthesia. In the second step6-12 hours later we have currataged the same tract or sinüs, by bushon curretes,1-4 mm in size.If the pitzs have been created in the a retracting fossa,it has been excised and sewed,to prevent reentries of hairs. Then we have washed the tract or sinüs by Povidone iodine complex and filled the tract with a soluble antibiotic pomad, like Furacinand dressed the region with an overcompressing gauze,for two days,and have limitted hard working or hard movements to collaps the residual cavity and for prevent seroma colection for four days. On the second or third day,we have changed the compressing dressing with a loose dressing or leave open ,but cover with a wound poudr to keep dry the regionand adwised him to change it two times in a day. On the 5 th or 7th day again we have invited him take off the dressing and the sutures if had been inserted.We heve insisted all patients, keep clean and dry the intergluteal region and never to sit in semilaying position, to prevent the new pitz formations.
THE ADVANTAGES OF THE METHOD
1-AgNO3 instillation has widened the pitz or entries,so fascilitated the entry of curretes into them and work more easily.
2-It have indicated all relating pitzs, particularly the very narrow or obilterated with ceratin plug,that may would have been overlooked, otherwise.
3-It chemically has cauterized and liquified the pyogenic granulating tisue inside the tracts ,so loosened the sticking hairs against the wall in the tractsthen surely then it was quiet easy to curratage and wash away the debris easlyneeding no insicion ,nor excision of the tract or sinüs
4-It has mininized the opeartive time and bleeding,
5-It can be induced under local aenesthesia by buffered Jetokain (Lidocaine %0,25) 1/10 NaHCO3.
The procedure was completed by the induvidual 2-3 mm microexsicions of the hair entries(pitzs),and leaving them unsewedbut excising and sewing the resembling dimples or fossae, by a single continuing 5/0 Trofilen suture subcutaneously at once leaving free the suture ends untied due to protect the wound edges from suture injury.
In the very fresh or early pitzsAgNO3 instillation gave pain,due to lacking of fibrous fistulary capsula yet and in very old or delayed, Grade 4 -5 cases there was no use of AgN03 instillation ,because of the epidermal epithelium invaded into the opening in the deep clfet.
Wheras it was unable to cauterize the scleroized Grade 4 pilonidal tracts by %30 AgNO3 solution in approximately 22% of so cases,because they were all delayed cases for more then 5-10 years,and have been transformed to be an unpleasent apocrin gland enfection or supurative hidradenitis with laterally extending tracts through out of the sacrococcygeal area like surrounding surrounding buttocks with intraepitelized fistulous tracts or scleroized entries and sometimes exits.Many tracts were have been longitudinaly insircled by a fibrotic and edematous surrounding tissue due to chronical infection, and also, they have been invaded by a resisting cutaneous epithelium, insidely, wich permanently keep the tracts openso impared the the healing of the treated
tracts,even of AgNO3 instillationbecause of the insisting of the intrafistulous dermal epithelium.
In the Grade 4 pilonidal sinüs disease, so it was better to inscice and unroof the tracts,and lay open them simplywhere the insiced edges, all have been epitelized by the aid of the epithelium in the involved tracts and surrounding skin,in two weeks or so. If the buttocks have been invaded vigorously with the pilonidal diseaselaying open wolud not bee enoughso ,large excision and flaping was necessary.
One fourth of the cases were in cystic form ,that having no exit,but only entry. If have simply excised the membraneous or fibrous capsula and capitonated the residual cavity with 2/0 Vicryl,and closed the insicion with 2 or three 4/0 Trofilen sutures,if they were not supurated.If they were supurated or with abscess formation,we have drained the abscess cavity trough an apical insicion and have left open for drainge until healing by itself but have treated every existing hair entry(pitz) ,which were found always distaly in a small dimpleand have sewed with one or two 5/0 Trofilen stitches,or left unsutured, wich havebeen enough for spontaneous healing for many 2-3 mm excised pitzs. At the end of the 4 or 6 days,we have taken off the any inserted stiches where all the insicions have healed already.All the pateints have been advised to keep clean the site and to sit on the buttocks but never on to the sacrum.The morbidity was aproximately %7 and the reccurence rate was only %3 in a 6 months and %5 in a year.
Almost all of the delayed but untreated chronical supurating grade 4-5 cases or unfistulated pilonidal tracts(sinüs formations), showed acceserbating and resisting abscess formations until perforating trough out the neighboring skin ,or some have extended in to the deep tissues like the wertebrates,the rectum, the scrotum, the urethra, the pubis, the groins, even as in our a 67 year aged case, into the urinary vesica, wich have induced a bleeding vesical malignant toumor by the end of the 25th year of disease .It may be better to classify those vigorous cases, that have been extendet out of the region as Grade 5,which were inoperable and untreatable by AgNO3 ,or by curattageso we now try to treat them by Isoretionin tablettes (Roaccutane) and Clindamycin,for a year and draining the abscess formations however it is al concervative method,but better to do notting.
In conclusion, treatment of pilonidal sinus disease in selected cases is a good alternative, minimal invasive method with encouraging results. The need of 6-12 hours intervall between instillation of AgNO3 and curratage may give reluctance to the very busy surgeons and patients. Also painful instillation in some fresh or verly cases and some insuffiency in the late grade 4 cases, needs to limit the method for grade 2 and 3 cases.
|


